Arq Bras Cardiol: Imagem cardiovasc. 2025; 38(1): e20240133
Prosthetic Valve Endocarditis: A Multidisciplinary Challenge
DOI: 10.36660/abcimg.20240133i
Clinical case
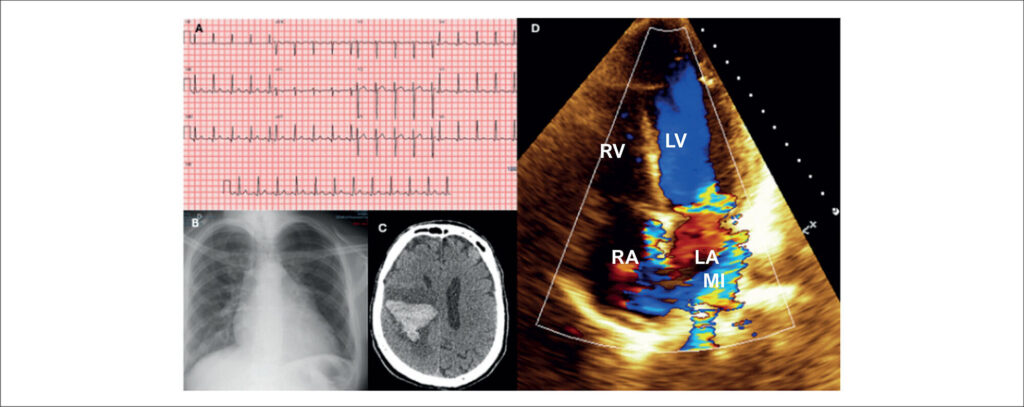
We report the case of a 55-year-old male patient who was admitted to the hospital in July 2019 with sudden left hemiplegia, mitral systolic murmur 4+, and aortic systolic and diastolic murmurs 2+. He had a history of aortic valve replacement in 2015, with a mechanical prosthetic aortic valve (PAV) due to infective endocarditis (IE). Cranial computed tomography (CT) revealed a right frontoparietal hematoma (), and blood tests revealed hyperglycemia and elevated C-reactive protein. His electrocardiogram (ECG) showed sinus rhythm with repolarization abnormalities (), and a chest X-ray showed cardiomegaly +/4 (). Transthoracic echocardiography (TTE) showed preserved function, thickening of the mobile elements of the mechanical PAV, mild double aortic lesion, pseudoaneurysm of the mitral-aortic intervalvular fibrosa, and important eccentric mitral regurgitation (). Blood cultures were requested, and ceftriaxone 4 g/d and teicoplanin 800 mg/d were started. Transesophageal echocardiography (TEE) showed vegetations on the ventricular side of the mechanical PAV leaflets and periprosthetic abscess (). Group B Streptococcus agalactiae was identified, and surgical treatment was indicated after 4 weeks due to cardiovascular stability and hemorrhagic stroke.
On day 22 of hospitalization, the patient presented pulmonary congestion and respiratory failure. Repeated TTE revealed partial loosening of the mechanical PAV and severe periprosthetic leak. Emergency surgery was performed to clean and replace the mechanical PAV with a biological PAV, without mitral valve approach. Culture of the explanted prosthesis revealed no bacterial growth.
[…]
Keywords: Endocarditis; Heart Valve Prosthes; Multimodal Imaging
408