Arq Bras Cardiol: Imagem cardiovasc. 2023; 36(2): e361
New Application of FFRCT in Clinical Practice: Evaluation of Interarterial Anomalous Coronary Course
Discussion
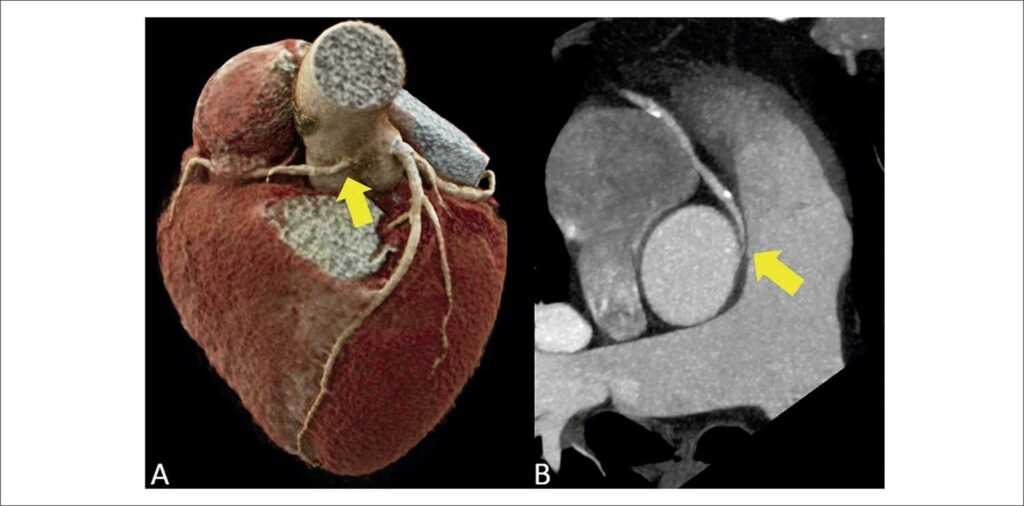
Anomalous origin and course of coronary arteries are rare congenital heart diseases, affecting less than 1% of the general population., Anomalous coronary origin with an interarterial (suprapulmonary) course is characterized by the course of the coronary artery between the ascending aorta and the pulmonary artery trunk, most commonly involving the right coronary artery., Most individuals are asymptomatic, but, among symptomatic patients, chest pain and dyspnea on exertion are the most prevalent complaints. There is also an increase in rates of arrhythmia, sudden death, and acute myocardial infarction., Sudden death is the main complication of this anatomical variant, occurring in approximately 30% of patients.,, In these cases, the narrowing and stretching of the anomalous ostium, mainly during physical exercise and in stressful situations, with consequent reduction in coronary flow, is the substrate for potentially fatal ischemic alterations.,, Since electrocardiogram, in most cases, does not reveal ischemic alterations, diagnosis is generally made through an incidental finding on imaging exams. These exams are of great importance, especially coronary CTA, which, in addition to being a non-invasive exam with high negative predictive value, allows detailed anatomical visualization (angle of the origin, presence of intramural trajectory in the aorta, degree of ostial/proximal luminal reduction) and the correct classification in relation to the pulmonary valve plane (suprapulmonary versus subpulmonary).,,
Recent studies have demonstrated that coronary CTA is an accurate test for identifying myocardial ischemia through FFRCT, when compared to invasive measurement (iFFR) by coronary angiography.,,, The detection of ischemia in coronary CTA is of great importance in decision-making, mainly in plaques considered moderate (50% to 69% luminal reduction) or when there is diagnostic doubt, reducing the number of unnecessary referrals to coronary angiography in cases without ischemia on FFRct.,, Due to the excellent accuracy between the methods in the analysis of a coronary tree without anomaly, the applicability of the method in the context of coronary anomaly has been extrapolated., Our group applied the most current version of a tool for calculating FFRCT currently available only on a research platform developed by Siemens Healthineers (cFRR, version 3.0.0) in the clinical case described. This research tool is available for installation on standard configuration computers, and it uses artificial intelligence tools, with reduced processing time. Currently, commercially available options require the step of sending images in DICOM format for processing in specific centers, with delivery of results at least 24 hours after the images have been sent., The research tool used in this clinical case has advantages, such as fast processing time on standard configuration computers in the analysis room and use of tomographic images from the standard routine protocol, without requiring the addition of a specific protocol or a higher dose of radiation, without the use of stressors., This tool, in general, has some limitations, such as difficulty in defining the coronary borders in the presence of excessive calcification, and the need for high-quality images, without movement artifacts, for adequate automatic detection of the central luminal line and the lines that delimit the coronary borders, allowing adequate calculation of FFRct. It is important to emphasize that this tool distinguishes the interarterial pathways associated with ischemia, considering only the flow obstacle during rest, without estimating the risk of ischemic events associated with dynamic changes secondary to intense exercise. Use of this tool is scarce in the literature, and it still does not have a robust body of evidence. Nevertheless, in the clinical case described, the FFRCT tool was applied in a context different than what is usual, where luminal reduction was not determined by coronary atheromatosis, but by ostial angulation and compression of the proximal segment of the anomalous interarterial pathway. The ischemic response was considered a parameter of poor prognosis; subsequently, the confirmatory invasive functional test (iFFR) was indicated to assist in the therapeutic decision.
[…]
463