ABC Imagem Cardiovasc. 2025; 38(3): e20250064
Tricuspid Valve: Anatomical Basis and Patient Selection Criteria for Transcatheter Structural Interventions
DOI: 10.36660/abcimg.20250064i
Abstract
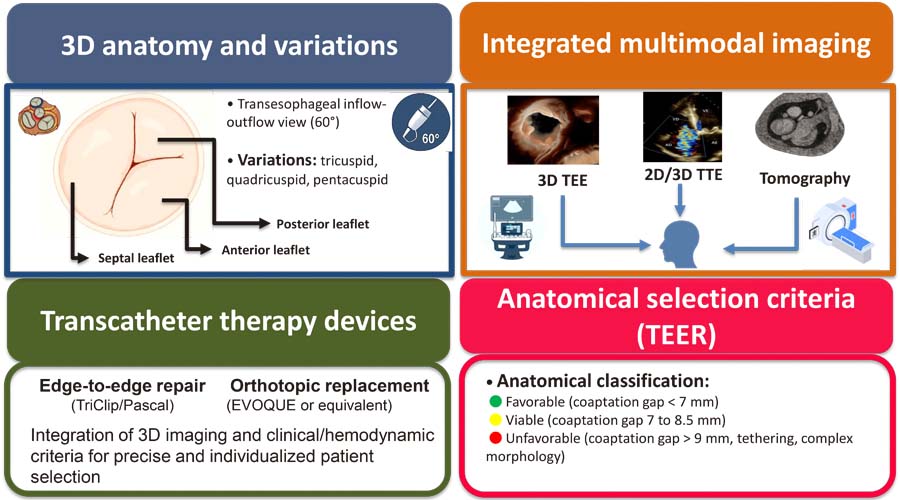
Tricuspid regurgitation has been recognized as a relevant clinical entity, with a direct impact on morbidity and mortality. Recent advances in multimodal cardiovascular imaging have promoted more detailed anatomical and functional assessment of the tricuspid apparatus, guiding the indication and planning of transcatheter interventions. To provide a review of the anatomical basis of the tricuspid valve and discuss echocardiographic and clinical criteria for selecting candidates for transcatheter therapies. This narrative review of the anatomical variability of the tricuspid valve and its subvalvular apparatus incorporates recent recommendations from echocardiography societies and clinical evidence. Special emphasis has been given to three-dimensional echocardiography, transesophageal echocardiography, and computed tomography for morphological and functional characterization of tricuspid regurgitation. Contemporary evidence has demonstrated that up to 45% of patients present with non-classical morphologies (quadricuspid or pentacuspid valves), which impact the viability and outcomes of edge-to-edge repair. The integration of three-dimensional echocardiography enhances accuracy in grading regurgitation severity, enables precise measurement of the vena contracta area, and assists in device selection. Clinical factors including right ventricular function, pulmonary artery systolic pressure, and the presence of intracardiac devices also influence patient selection. Appropriate selection of candidates for transcatheter tricuspid valve therapies requires a systematic approach with integrated application of imaging methods and clinical parameters. Detailed echocardiographic characterization of leaflet morphology, coaptation gap, and annulus geometry is crucial for planning the procedure, selecting the device, and predicting outcomes.
701